
Ireland has a big problem with undetected cases of stubbornly high cholesterol in the population that is leading to unnecessary deaths due to heart attack or stroke, according to a leading cardiologist.
Prof Vincent Maher, who is based at Tallaght University Hospital, Dublin, highlighted the issue after a study of lipid levels found "high levels of untreated cholesterol among Irish adults".
Abnormalities in cholesterol levels are proven to cause cardiovascular disease, which accounts for 32 per cent of all deaths in Ireland; “making it the greatest cause of mortality in the country,” he pointed out.
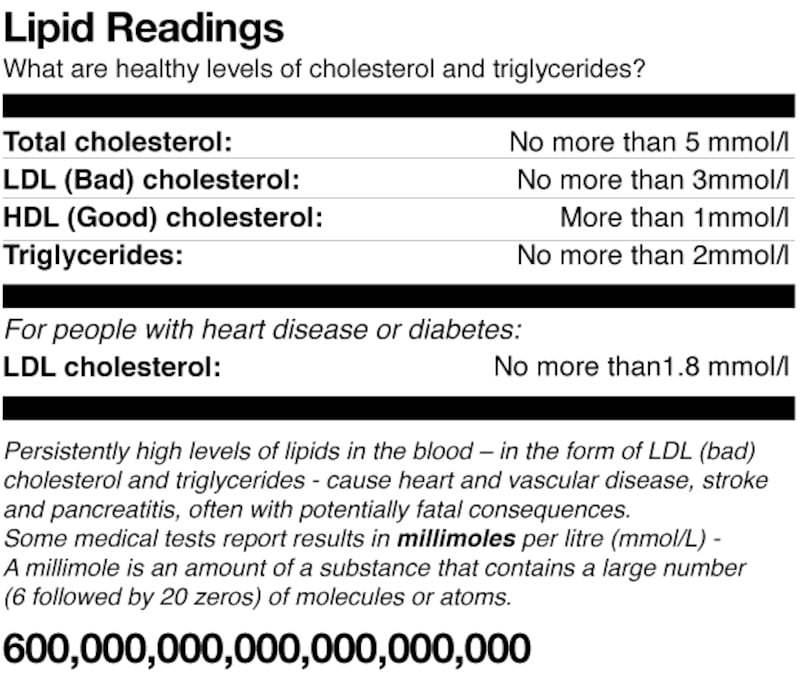
The research reveals 60 per cent of those tested had some form of “lipid abnormality” due to high cholesterol or high triglycerides in their blood – cholesterol, a normal constituent of cells, causes problems if there are high levels in the bloodstream.
The study, undertaken as part of a cholesterol-awareness campaign in July 2017, is published in the Irish Journal of Medical Science. Random testing took place in five counties – Leitrim, Westmeath; Kerry, Mayo and Kildare – while 110 of those tested were men and 149 were women; all aged between 18 and 92 years.
There was no doubt about high cholesterol being “a causative factor” in cardiac and vascular disease, he said. Low-density lipoprotein (LDL), or “bad” cholesterol, attaches to artery walls due to atherosclerosis; a build-up of fatty deposits in that leads to heart attacks and strokes.
In spite of this, Prof Maher said there has been no “whole of population” study conducted in Ireland, other than “snapshot studies of the over-50s” which were not representative of the extent of the problem.
Members of the Advanced Lipid Management and Research (ALMAR) team at Tallaght Hospital obtained fingertip blood samples to perform “a full lipid profile” participants in the study.
“There are too many people with high LDL cholesterol . . . not all of them are going to get heart disease but they need to be assessed. High cholesterol is a warning sign, not necessarily cause for alarm. It suggests further evaluation should be carried out,” he said.
Awareness of cholesterol risk was low among participants, with most people being unaware of their cholesterol level or that different types of cholesterol exist.
“The results also highlight low levels of awareness, which is very concerning. People did not know the difference between good and bad cholesterol. Given the evidence that high LDL causes heart disease, it was also of concern that “they are unaware of the risk”, he added.
LDL cholesterol is “lousy, lethal and lays it into arteries”, while HDL cholesterol is the “happy, healthy, hover”, he advises patients.
Those with high LDL, such as those with a genetic predisposition, could be susceptible though they may be slim and fit and say to themselves, “there’s no way I could be at risk of heart disease”, he said.
Environmental factors such as poor diet; lack of exercise, hormones, weight and stress levels together with familial cardiac risk factors can increase cardiac risk and risk of pancreatitis due to high triglyceride levels, he said.
There has been a steady decline in cardiovascular mortality in Ireland, with over 20 per cent of that attributed to cholesterol reduction. “Despite this, heart disease accounts for 32 per cent of all Irish deaths. While these observations are not fully representative of the national population, they do highlight significant lipid abnormalities in the Irish population.”
To ensure further decline in cardiovascular disease, a representative sample of lipid levels in the population should be conducted at least every five years, Prof Maher said. “The main importance of our finding was that significant lipid abnormalities were identified in Ireland many of which were previously undiagnosed.”
Studies have shown that even if identified, treatment levels were inadequate. “Therefore, screening together with education and knowledge of appropriate lipid targets will be necessary to correct this major atherosclerotic risk factor,” he said.
There is no national screening strategy or dedicated resources in hospitals, in primary care or the community “to diagnose and treat cholesterol-related disorders effectively so as to reduce cardiovascular risk”.
As there is evidence of disease that is preventable in most cases, this is equivalent to saying “we are ignoring diabetes”, Prof Maher contended.
He is trying to establish a dedicated ALMAR centre at Tallaght Hospital to treat patients with challenging cholesterol disorders; to facilitate family screening and “refine patients’ diagnoses” following specialised investigations. A prototype, which would cost about €100,000 a year to run, could then be replicated around the country as go-to-places for patients with proven disease and who are facing challenges in trying to reduce their cholesterol.











