
It has all the makings of a perfect storm: an overloaded health service that struggles to fill posts; a pandemic-weary workforce still dealing with massive patient backlogs; older staff who want out; and younger ones looking for a better work-life balance.
Figures tell some of the story:
391: the number of visa applications granted last year to Irish doctors to work in Australia.
837: the number of consultant posts not filled on a permanent basis;
0: the number of applications received for nine highly remunerated consultant posts that were advertised last year;
4,787: the number of older people left without a carer due to chronic staff shortages.
For the first time in many years, the health service has money to spend. It is recruiting staff in record numbers – including 133 permanent consultants since last May. But this isn’t happening fast enough to meet the needs of a growing, ageing population and the challenges of massive backlogs.
“We don’t struggle to get good people into the health service. It’s just that there aren’t enough good people out there,” says Anne O’Connor, HSE chief operations officer.



The challenge of recruiting and retaining health staff goes a long way towards explaining persistent long waiting lists. A lack of consultants means fewer clinical decision-makers. Too few care staff means older patients cannot be discharged from hospital even though they are well.
Staffing gaps heap further pressure on workers forced to fill them. This in turn makes it harder to hold on to staff, for whom emigration or retirement increasingly look like attractive options.
Shortages of doctors and other key staff have consequences for patients. Every unfilled post means fewer patients seen, fewer operations carried out and fewer clinical decisions made.
Could the five unfilled posts in BreastCheck last May be a reason for the one-year delay in screening women following the interruptions caused by the pandemic? Are the 27 empty posts in Children's Health Ireland a factor in the running sore of long waiting lists for scoliosis operations? Are delays in genetic services for infants linked to the failure to appoint a professor in genomics medicine, despite an international search?
Overall, 837 consultant posts are not filled on a permanent basis, but the scale of the problem varies hugely across the country and across specialities.
Recruitment in some urban areas is hampered by the fact staff cannot afford to live there
Dublin teaching hospitals with plenty of doctor training posts are less impacted because of opportunities for advancement. These are big hospitals anyway, so there is scope for staff to share the extra load caused by a few vacant posts.
In contrast, smaller, level 3 hospitals outside the capital, with fewer training opportunities, struggle to get and keep staff. Filling or not filling a post can be the difference between providing a much-needed service or not providing it at all.
“It depends on what the job is and where it is,” says O’Connor. “There are parts of the country where it is always easier to recruit certain disciplines than others. Certain disciplines want to be close to the mothership of the big cities and the big teaching hospitals.”
Recruitment in some urban areas is hampered by the fact staff cannot afford to live there.
Mental health services
By sector, mental health is worst affected, with 63 psychiatry consultant posts unfilled on a permanent basis, some vacant for many years.
The HSE has a clear problem with recruitment, says Dr Niamh Humphries, a senior lecturer at the RCSI graduate school of healthcare management. "If you speak to the people doing the work it feels as though they're working in a health system that's understaffed – that there's not enough people on the ground to do the work coming at them.
“Hospital doctors are really struggling with workload and working hours, and with work-life balance. The service is understaffed and overstretched. There are too few people doing too much work.”
These underlying problems have only been intensified by the two years of the Covid-19 pandemic, she adds.
But isn’t the health service spending record amounts of money and recruiting more staff than ever before?
“You can measure it by how much money is spent or how many extra people are recruited but if that isn’t making a difference to the people on the front line, then I’m not sure they’re the right measures. If these jobs are not attractive, if staff are unhappy, they’re going to leave.”
High levels of churn – about 7 per cent a year – appear to bear out this analysis. The HSE has to recruit more than 9,000 staff each year just to stand still.
'We need to encourage diversity in what we do. Doing 100 per cent of the same job for 30 years can lead to burnout'
Recruitment challenges in health have many causes, according to infectious diseases consultant Prof Mary Horgan, including a tradition of medical emigration, increasing burnout and changing expectations among staff.
The health service needs to move away from “one size fits all” medical jobs to more flexible working, she argues.
“Working conditions, not having to work long hours, work-life balance – these are more important to a younger generation. They have a different perspective.
“We need to encourage diversity in what we do. Doing 100 per cent of the same job for 30 years can lead to burnout.”
Horgan has taken the opportunities for change over a varied career. She spent seven years working abroad, is in her second year as president of the Royal College of Physicians of Ireland and joined the National Public Health Emergency Team last year.
While most health professionals don’t have “the luxury” of working from home generally, she says, many would like to work three or four days a week.
“Because we need these highly skilled people, the system needs to adapt to their needs. It is better to have a doctor happy working three days a week than not at all.”
Humphries says recruitment and retention of staff are “absolutely interconnected – you can’t look at one without the other”.
In her interviews with staff, working conditions come up the most, along with long hours and heavy workloads and “not being supported to be the best they can be”.
As a result, younger doctors are encouraged to look at emigration, while older ones consider retiring earlier.
“People want work life-balance. They want to be able to go home at the end of their working day not completely stressed out, to have time and energy left to spend with their loved ones.”
European directive
The HSE reports 98 per cent compliance in hospitals with the European Working Time Directive, which limits the length of a doctor’s shift to 24 hours, and 84 per cent compliance with the 48-hour working-week rule.
But Humphries says the protections the directive was supposed to provide haven’t translated into the everyday working experience of hospital doctors.
“When you talk to doctors on the ground, they say they are not working hours that are compliant, or having break times or lunch times or any of the protections in the [directive].”
“There’s a massive disparity between what the HSE is saying and the lived experience of junior doctors,” says Dr John Cannon, chairman of the non-consultant hospital doctor committee of the Irish Medical Organisation. “The system is resource-poor, it is adversarial and so it sets people against each other. You end up working unfeasibly long working shifts and experiencing the heartbreak of explaining delays to patients, day after day.”
Upwards of 1,000 junior doctors are expected to attend an online emergency meeting on Monday evening as unrest surges among non-consultant hospital doctors. “These issues were shelved during the pandemic in the national interest but now doctors’ deep-seated anger is coming to the surface, along with extreme fatigue after the last two years,” says Cannon.
'We tend to have everybody wanting to move up and move on, but the core duties, such as nursing a ward of older people, they're harder jobs to fill'
Thirty per cent of the HSE’s 150,000 staff work part-time. While the organisation will support hybrid working, O’Connor says this is less feasible in patient-facing areas providing 24-7 cover.
She points to the job security and career progression enjoyed by staff. “Ultimately, the health service is a fantastic career pathway for people who have any kind of interest in it.”
She questions whether the focus on points in the Leaving Cert means “we end up with the right kind of people for caring jobs and not just the academically bright”.
“We tend to have everybody wanting to move up and move on, but the core duties, such as nursing a ward of older people, they’re harder jobs to fill.”
O’Connor herself will be leaving the HSE soon to take up a senior role with VHI.
‘Moving parts’
Recruitment problems are aggravated by slow-moving processes – it can take up to two years to appoint a permanent consultant.
“One of the problems about recruiting into the health service is that there are a lot of moving parts – public and private hospitals, the training colleges – and the HSE doesn’t have control over all of them,” says one experienced medical recruiter, speaking on condition of anonymity.
“I have a doctor, who has already worked in Ireland, who has been waiting at home for three months for his work permit to come through. It’s absolutely insane.”
The HSE says more than 500 consultant posts were approved last year, and training places are being expanded in many areas. For instance, the number of Child and Adolescent Mental Health Service specialists trained is being increased from three or four to about 12. Advanced nurse practitioners are also being trained and appointed in greater numbers.
With a retirement cliff approaching in general practice, the number of GP training places has been increased from 193 in 2020 to 233 this year, and is projected to increase further to 351 in 2026.
If anything the reliance on agency staffing is even more pronounced in nursing
The focus around unfilled posts is often on consultant positions because the system is hierarchical and consultants play a key role in making clinical decisions in hospitals. But the difficulties around recruitment extend more widely.
If anything the reliance on agency staffing is even more pronounced in nursing, with the Irish Nurses and Midwives Organisation reporting some wards are 95 per cent staffed by agency workers.
As for the role doctors play in clinical decision-making, Horgan says she is a “huge advocate” of other healthcare workers taking on senior roles. The pandemic accelerated this transition by giving pharmacists new responsibilities, while physiotherapists managed patients’ oxygen needs in intensive care.
Ireland has one of the lowest numbers of consultants relative to population of any country; conversely, we are oversupplied with junior doctors. Compared with Australia, for example, Ireland has almost 50 per cent fewer consultants and about 30 per cent more non-consultant hospital doctors.
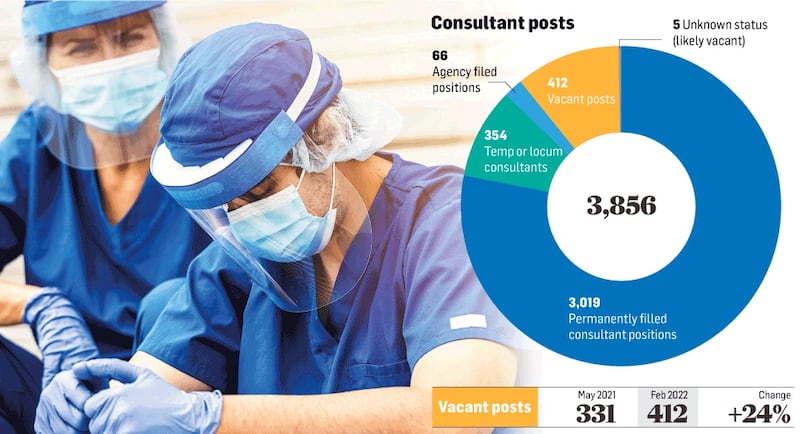
But of the 3,856 posts, 412 are vacant, according to latest figures obtained by the Irish Hospital Consultants Association, up significantly from the 331 recorded only last May.
The HSE makes the point that three-quarters of vacant posts have been unfilled for less than a year, and many are newly approved posts with recruitment procedures in the works.
Yet of the 3,439 posts regarded by the HSE as filled, 420 are occupied by temps, locums or agency staff. These arrangements can vary from very short-term contracts to longer-term arrangements that are rolled over from one year to the next.
And due to these gaps, 3 per cent of specialist posts are filled by doctors who are not on the specialist register.
Non-EU trained doctors
Traditionally, Ireland has made up for a shortage of domestically trained doctors by importing them from other countries. Given the global labour shortage in medicine, however, this group of doctors is increasingly looking at options elsewhere. Largely excluded from training opportunities to become consultants, and confined to short-term contracts, non-EU trained doctors in Ireland are becomingly increasingly restive.
"More than 95 per cent of international doctors are not on a training scheme. Most of us experience visa difficulties and are on short-term contracts," says Dr Liqa Ur Rehman from Pakistan, who has been campaigning for improved conditions. "In general, working conditions are hostile. You can easily be victimised, and bullying is a big issue."
'Doctors are on short-term contracts for a long time in their career, and that builds in vulnerabilities'
Working on a succession of short-term contracts can mean having to relocate every six months, to find a new house to rent and new schools for children to attend, he says.
“If people don’t have progression opportunities while working in Ireland, they won’t stay,” says Humphries. “Doctors are on short-term contracts for a long time in their career, and that builds in vulnerabilities.”
The Government has changed the system to allow for a two-year work permit, so doctors don’t need to change work permits every time they move hospital. In March, non-EU doctors were given quicker access to the right to work without a permit as well as spousal work rights.
Ur Rehman continues to campaign for greater recognition of the prior qualifications of non-EU doctors, and of their time spent working in the Irish system.
Ultimately, the solution lies in recognising that there is a problem, says Humphries, and to “pay more attention to the workforce as we move out of the pandemic”.
“You have to put health workers front and centre in any recruitment policy. At the end of the day, they’re the people you want to fill the posts.”
















